4. Understanding Disability: Beyond a Checklist
Expanding what counts as disability
Many of us have been taught to associate disability with something specific, easily noticed, and stable over time. This narrow understanding is reinforced by the images and symbols we are surrounded by.
But this is a limited and narrow version of disability that leaves out a great deal.
For example, the International Symbol of Accessibility (below) has become widely used to represent disability and access needs. While it plays an important role in identifying accessible spaces and supporting disability rights, visually it reflects only a portion of the disability community.

Image Description: A square graphic showing the International Symbol of Accessibility. The background is a solid blue. In the center, a stylized white figure is seated in a wheelchair. The entire square is framed by a thin white inner border and a blue outer border with rounded corners.
The wheelchair symbol and disability representation
The International Symbol of Accessibility was developed in the late 1960s and has become one of the most widely recognised disability symbols globally. It is often associated with physical disability, particularly mobility-related disabilities.
More recent work, like this Disability Symbol initiative by Hope Hoffman and Jessica Oddi invites a broader reimagining. This project proposes a symbol designed to represent disability as diverse, evolving, and interconnected rather than tied to a single body, condition, or experience.
Learn more: The Disability Symbol
Disability is far more common, and far more varied, than many of us have been led to believe. According to Statistics Canada’s 2022 Canadian Survey on Disability:
- 27% of people aged 15+ in Canada identify as having one or more disabilities*
- Among youth aged 15–24, the rate is approximately 20% (Statistics Canada, 2024).
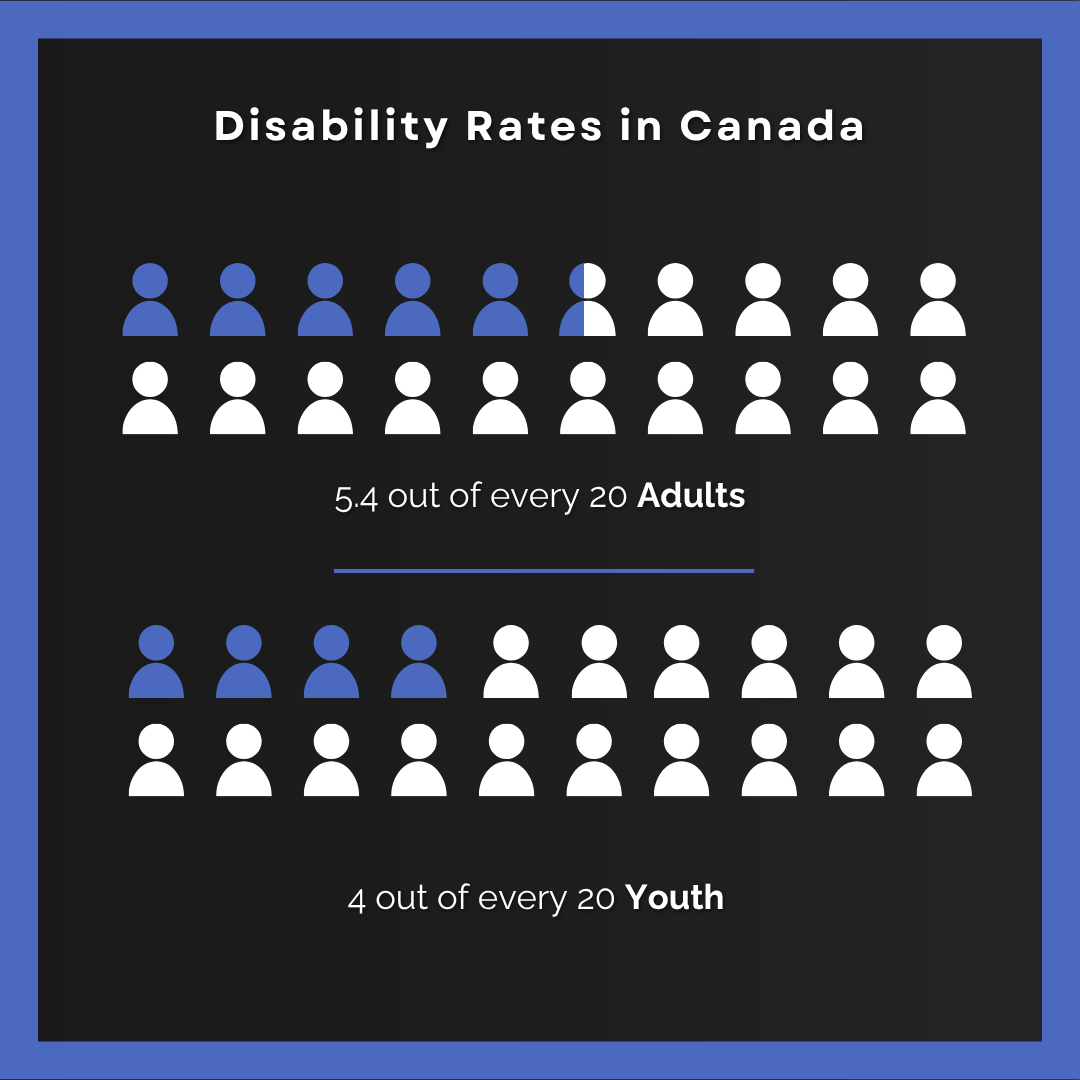
Image Descriptions: A dark-background infographic titled “Disability Rates in Canada.” Two rows of simplified person icons visually represent proportions. The first section shows adult figures, with 5.4 out of 20 icons highlighted in blue to indicate the proportion of adults with disabilities. The second section shows youth figures, with 4 out of 20 icons highlighted in blue.
*Note: This data captures people living in private households only and excludes disabled people living in care, who are unhoused or live in institutional settings. It also likely does not accurately reflect Indigenous people with disabilities living on reserve.
These data challenge a common assumption that disability is a small or niche population. Disability is already part of our programs, our teams, and our communities, whether it is named or not, and whether we know it or not.
A Vast and Varied Experience
If disability is more common and more varied than we’ve been taught, then we cannot always rely on what we can easily notice, name, or diagnose to understand who is disabled or who may need support (Valeras, 2010). These categories can be useful, but they are not fixed or complete. Many people move across them over time, and the following list is by no means exhaustive:
- Physical disabilities (e.g. mobility, chronic pain, coordination)
- Sensory disabilities (vision, hearing, sensory processing)
- Cognitive and intellectual disabilities
- Learning disabilities
- Mental health conditions and psychosocial disabilities
- Neurodivergence (e.g., Autism, ADHD)
- Chronic and episodic conditions (e.g. migraines, autoimmune conditions, long COVID)
- Acquired and congenital disabilities
- Visible, non-visible, and non-apparent disabilities that are subject to negative social attitudes and isolation
For some people, disability is consistent and named. For others, it is fluctuating, context-dependent, or not easily captured by a single label (Valeras, 2010). Even this list has its limits.
This means disability is not always something we can clearly put into a box If cannot always be categorized, identified, or defined.
Moving Beyond a Checklist
Given this range and variability, it is understandable that people look for clarity. They want to know:
- What should I say?
- What should I do?
- What should I avoid?
Or they feel they need to understand every diagnosis to respond appropriately. But a checklist approach will always be incomplete. It leads us to:
- rely on assumptions tied to diagnosis
- treat people with specific disabilities as a monolith (“I’ve worked with someone with this before…”)
- try to “figure people out” rather than get to know them
- respond based on expectations, rather than actual experience
A widely shared saying in Autism communities is: “If you’ve met one person with Autism, you’ve met one person with Autism.”
This principle extends beyond Autism. Within the same diagnosis, people’s experiences, strengths, and needs vary widely. They change across a lifetime, across a season, or even across a single day. For example, a student on crutches who suddenly can’t access stairs, someone recovering from illness or navigating fatigue, a person who doesn’t “fit” a category but still needs support to fully participate.
When access is treated as something you must qualify for, rather than something we can respond to, people get left out. A checklist simply can’t keep up with reality.
What matters most is our ability to stay responsive to real people, and to notice, check-in and adjust as we go.
Identity, Visibility, and Disclosure
As our understanding expands, another shift emerges. Disability is not just something a person ‘has’. It can also be a lived experience, a social position, and, for some, a meaningful identity (Valeras, 2010).
For many, disability, including those who may not identify as “disabled” but who have diverse access needs, this can be understood as::
- a lived experience
- a connection to communities formed around shared experiences and access needs
- a cultural and political identity
At the same time, not everyone identifies with the words ‘disabled’ or ‘disability’.
For some, claiming that identity can bring pride and connection. For others, it can carry risk, stigma, or unwanted assumptions, and for some, it is not an identity they claim at all.
When we put this together, something important becomes clear: disability is not always apparent, and it is not always disclosed.
Many people choose not to disclose, or may not feel comfortable doing so, for a range of personal and structural reasons, including stigma, bias, and uncertainty about how they will be perceived (Valeras, 2010). For parents and caregivers, previous experiences with exclusion, being told their child is no longer a ‘good fit’ for a program, or their child being treated differently once identified, all shape their decision to disclose.
Many people have access needs that must be met to participate fully but may or may not identify with the label of disability. This can include, but is not limited to people in Deaf, fat, diabetic, and ADHD communities, as well as those whose access needs shape how they move through spaces, systems, and communities.
We simply cannot assume who is disabled and who is not.
Disability In Theory
The way we understand disability influences how we respond to it. Models of disability have shaped how disability is defined, studied, and addressed and continue to influence how people think, act, and design spaces.
The medical model locates disability primarily within an individual body or mind. It often focuses on diagnosis, impairment, treatment, or cure. It reinforces the idea that the person is the site of the problem; that they are broken or need fixing (Haegele & Hodge, 2016).
“The problem is in the person, and the goal is to treat or fix it.”
The social model shifts attention outward. It highlights how disability is also created by environments, systems, and expectations, such as inaccessible spaces, rigid program structures, or narrow definitions of participation. While influential, the social model has been critiqued for not fully accounting for lived experience, pain, or intersectional realities (Haegele & Hodge, 2016).
“People are disabled by barriers, not their bodies or minds.”
Disability justice pushes this thinking further. It builds on earlier disability rights frameworks by centering intersectionality, collective access, interdependence, and the leadership of those most impacted by ableism and other systems of oppression (Sins Invalid, 2019). It recognizes that disability is also shaped by power, identity, and lived experience. It challenges whose bodies and minds are considered “normal,” whose needs are prioritized, and whose experiences are made visible or invisible.
“Disability is shaped by systems of power, and so is access.”
Disability justice also reminds us that disability does not exist in isolation. It intersects with race, gender, class, culture, and histories of colonization, shaping how people experience access, belonging, and exclusion.
Disability In Practice
If we understand disability as a natural and expected part of a vast human experience, not something to fix or solve, what does that ask of us?
It does not ask us to become an expert in disability, but it does ask us to examine our assumptions about:
- who is disabled
- how we might know if someone is disabled
- and what we believe that means
This does not guarantee that you will always ‘get it right’, it does make it more likely that your responses are grounded in the actual experience in front of you, rather than expectations and bias.
You have influence over the relationships and environments you help create, including:
- how you show up and connect
- how activities are designed
- how instructions are shared
- how flexible expectations are
- how participants are responded to in the moment
These choices shape who can participate, how people experience belonging, and whether barriers are reduced or reinforced. The same activity can be inclusive or exclusionary depending on how it is designed and delivered.
Rather than trying to figure people out, this work invites us to ask: What is within my sphere of control that could make this experience more accessible, inclusive, and responsive? Where might my biases and assumptions be getting in the way?
Because disability is vast, doesn’t fit neatly into categories, and is not always disclosed, then inclusion cannot depend on us assuming or on individuals always asking for what they need.
This asks us to shift to:
- design with a wider range of bodies and minds in mind from the start
- normalize conversations about needs and supports
- reduce the burden on individuals to disclose or advocate for themselves
Up Next
In the next section, we will explore how common ideas (storylines, stereotypes and assumptions) about disability take shape and how they influence what we notice, expect, and respond to.
Viewed 526 times